


Knee Injuries & Reconstruction
Ligament injuries
There are four main supporting ligaments of the knee. They connect the tibia and femur, and stabilise and guide the knee during motion. These ligaments can be injured during sporting activity or in other accidents, leading to pain, swelling, and potentially a loss of stability. The Anterior Cruciate Ligament (ACL) is one of the most commonly injured ligaments. Absence of a functioning ACL due to injury may manifest itself as the knee giving way, particularly during twisting movements.
ACL ruptures can be treated by either repairing the torn ligament or by reconstructing it.
ACL reconstruction
There are many potential graft choices in ACL reconstruction. Each has its pros and cons.
Hamstring tendons
This is the most commonly used graft in ACL surgery. One or two tendons from the inner aspect of the knee are detached and folded to make a graft. This is a very strong graft, and has excellent long-term results. It can be taken via a small incision on the inner aspect of the knee. It is well tolerated and in most cases hamstring function is not impaired.
Patella tendon with bone blocks
This graft is also commonly used. The graft is the middle third of the patella tendon, which runs on the front of the knee from the kneecap to the shinbone. It requires a bigger incision than for a hamstring harvest, and has been associated with pain on kneeling. It is an excellent option for a revision (re-do) reconstruction.
Allograft
This is sterilised graft material from a cadaveric donor, and as such there are no harvest-site problems for the patient. These grafts are inferior to fresh tissue, as they are weaker and take longer to incorporate. The re-tear rate of allografts is higher and there are also concerns with potential infection.
Other options
Quadriceps tendon: This involves taking a segment of the tendon above the kneecap, with or without part of the kneecap bone. It requires a larger incision on the front of the knee and can lead to weakness of the quadriceps muscles.
Synthetic ligaments: are appealing due to the lack of any problems with the harvest of tissue. However, historically they have had a high failure rate, often due to an inflammatory reaction within the knee. The newer synthetic ligaments rely on preservation of the ruptured ligament stump, and acts as a splint for healing.
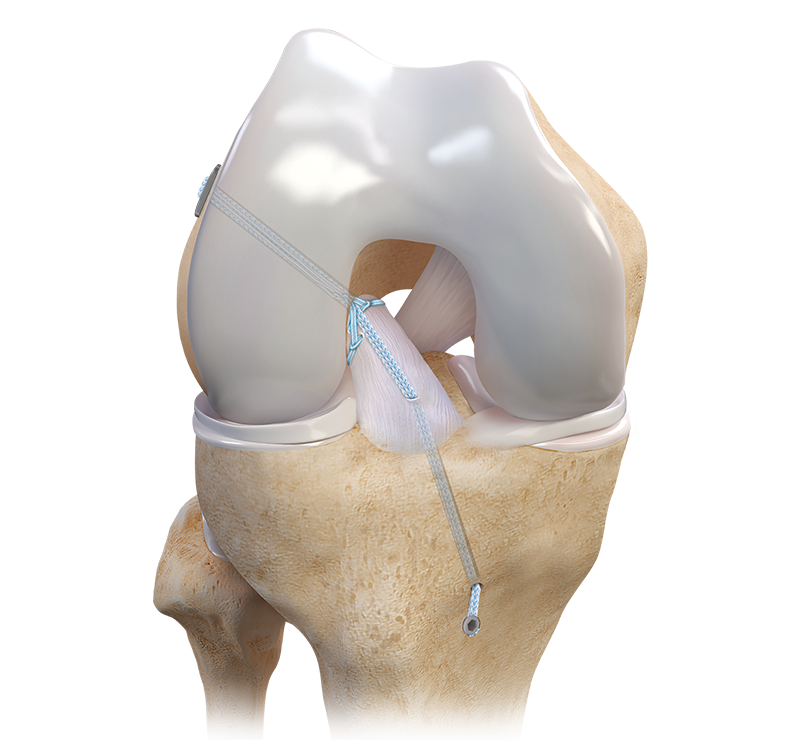
ACL repair
In some situation, it may be possible to repair the torn ligament. There are multiple factors that determine if a ligament is repairable or not. If it isn’t repairable (most often), a reconstruction is required. Sometimes this decision is made during surgery.
Dr. Van de Pol uses a suture technique that preserves the torn ligament and re-attaches it to the bone (mostly to the femur). The main benefit of repairing over reconstructing is that no donor tendons are required.
The majority of ACL injuries are not repairable and require a reconstruction.

My preferred technique
There are many ways to reconstruct a torn ACL and the used technique depends on the patients’ build and needs. My preferred technique for a primary ACL reconstruction is to use hamstring tendons from the same leg as the reconstruction. The tunnels are created using arthroscopy (keyhole surgery) and the graft is fixed in the femur and the tibia using screws that lock the graft in the bone.
Most often hamstring tendons are used for the reconstruction. Dr Van de Pol uses a single-tendon short graft techniques or a two-tendon standard length hamstring technique. Both techniques utilise screws inside the bone to secure the graft. Alternatively, quadriceps tendon or a bone-patella tendon-bone technique may be used if required.
Local anaesthetic is widely infiltrated around the knee, and there is no post-operative brace. Patients leave the hospital on crutches the day following surgery.